

There are a number of factors contributing to delayed eruption of a permanent incisor. If there is at least 3 mm of bone between the incisal edge of the impacted tooth and the oral cavity, spontaneous eruption could take much longer than usual, and treatment may be appropriate. Another factor would be crowding of adjacent teeth that are also on its way of erupting. The delay in eruption may allow adjacent teeth to drift into the empty space, which may further impede eruption of the unerupted tooth. If the timing of eruption is truly delayed in terms of both chronological and dental age, it is unlikely that the permanent tooth will erupt without orthodontic intervention.
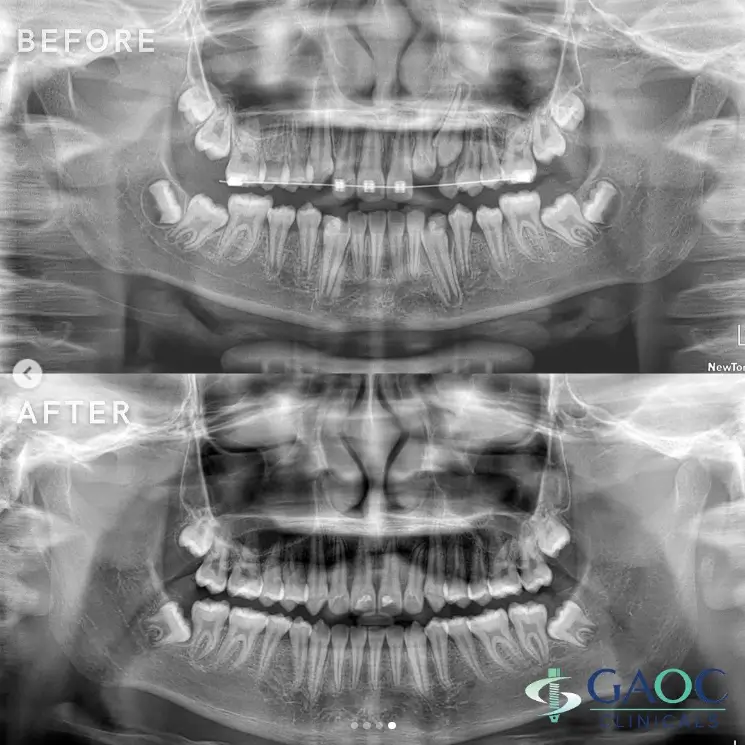
A 12-year old patient presented with an unerupted upper left lateral incisor. Location of the unerupted tooth was confirmed through panoramic radiograph and dental CBCT. Treatment recommended was exposing the tooth and using orthodontics for repositioning.
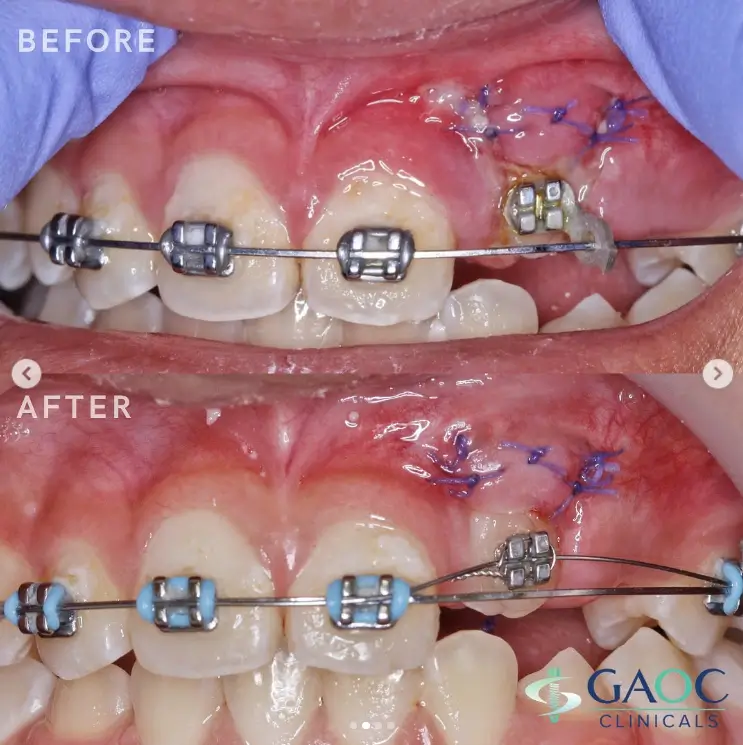
Local anesthetic used was 2% Lidocaine HCl with 1:100,000 epinephrine. Incision was made to expose the tooth with the soft tissue repositioned apically and sutured with 5-0 Vicryl (polyglactin 910). A metal bracket was bonded on the tooth whereby a rubber chain elastic was used to help traction it further downward. A working archwire in combination with a more flexible wire was used to pull the tooth into alignment. A light extrusive force is applied to guide the tooth into eruption. Continuous routine orthodontic adjustments were done and the entire treatment was done in 24 months.
#GAOCclinicals
#GAOCdental
#TheBenchmarkOfBrilliantDentistry


